
LLMs in evidence workflows: the new bottleneck is traceability - not speed
- FRESCI TEAM
- May 14
- 5 min read

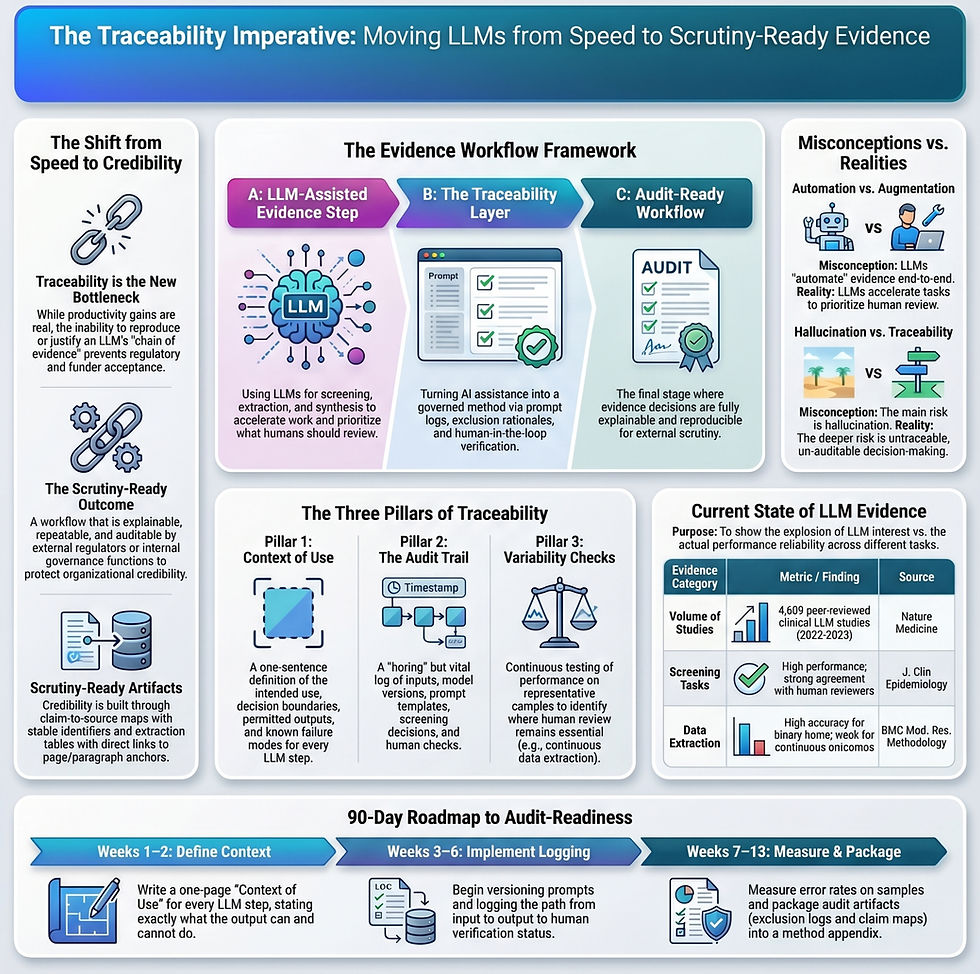
LLMs are entering evidence workflows faster than most biomedical teams are redesigning those workflows for scrutiny. That is the real strategic problem. The risk is not simply that a model will hallucinate. The risk is that a team will use AI inside screening, extraction, synthesis, or evidence mapping and later be unable to explain what changed or whether the result is reproducible.
The best available 2026 evidence supports a narrow but useful conclusion. LLMs can help with some structured evidence tasks, especially earlier-stage review work such as screening. But the closer a task gets to judgment, extraction fidelity, and downstream decision consequences, the more governance matters. For regulator-aware teams, the competitive advantage is not "more automation." It is traceable automation.
WHY IT MATTERS NOW
Many biomedical organisations are already using LLMs informally to accelerate evidence work: triaging abstracts, drafting summaries, extracting endpoints, matching claims to citations, and preparing internal briefing language. The bottleneck in most teams is no longer awareness. It is governance.
Evidence workflows are not judged the way marketing workflows are judged. They are examined by people who can stop, delay, or narrow a decision: regulators, scientific reviewers, funders, partners, procurement teams, diligence teams, and increasingly internal AI governance functions. Under that level of scrutiny, the operational question is not "did the output look plausible?" It is "what exactly did the system do, what boundary was it operating within, and can the result be repeated?"
That is why the FDA's March 2026 draft NAM guidance matters even outside NAMs narrowly defined. In fact, the same basic logic is increasingly relevant for AI-assisted evidence workflows. Novel tools may be welcomed, but only when their role, limits, and evidentiary behavior are intelligible.
WHAT CHANGED / WHAT THE EVIDENCE SAYS
The evidence base is exploding faster than it is maturing.
A Nature Medicine analysis published on 3 March 2026 reported identifying 4,609 peer-reviewed clinical-medicine LLM studies from January 2022 to September 2025. It also noted that among studies using real-world patient data, only a small share were prospective randomized trials. The article is not directly about evidence operations, but it captures the pattern clearly: publication volume grows first, while robust evaluation and decision-grade implementation norms lag behind.
LLMs appear promising for repetitive review tasks, but variable for high-judgment steps.
A Journal of Clinical Epidemiology systematic review, available online on 12 March 2026, synthesized studies of LLM performance across systematic-review steps. The high-level signal is directionally encouraging for some screening tasks, but the paper also supports cautious implementation and safeguards. That distinction matters. Promising for selected sub-tasks is not the same as ready to automate the workflow.
Extraction is where teams quietly lose credibility.
Even when screening looks strong, the workflow often becomes fragile at the next step: extracting structured, decision-relevant information consistently enough to support later claims or tables.
A BMC Medical Research Methodology paper published on 14 January 2026 tested LLMs for RCT data extraction and reported stronger performance for some binary extraction items and weaker performance for continuous outcomes. It works on some fields is not a deployment rationale. It is a design constraint. Teams need to define which fields are suitable for machine assistance, which still require full human extraction, and what verification standard applies to each.
Just so you know, there is a big but to consider here. Most of these papers were looking at studies that looked at older AI models, not the one we are currently using today.
STRATEGIC IMPLICATIONS
This is the point where a technical capability becomes a strategic decision. If LLMs touch your evidence workflow, the relevant question is not whether the model appears sophisticated. The relevant question is whether the workflow still behaves like a governed method.
TREAT EVERY LLM STEP AS A GOVERNED METHOD
FDA's press announcement on the draft NAM guidance explicitly frames validation in regulator-readable terms, including Context of Use, technical characterization, and fit-for-purpose logic. That language translates well. An LLM step in evidence work should be described the same way: what it is intended to do, what decision boundary it sits within, and what failure modes the team is controlling.
If a team cannot write a one-sentence Context of Use for an LLM step, it probably does not yet understand the operational risk of using the tool in that step.
BUILD AUDIT ARTIFACTS BEFORE YOU SCALE USAGE
Most organisations adopt AI in evidence work in the wrong order. They expand usage first and only later ask how the work will be documented. That sequence creates avoidable risk.
An LLM-assisted workflow should produce artifacts that a third party can interpret without insider context:
a claim-to-source map with stable identifiers
an extraction table with traceable source anchors
a log showing which steps were machine-assisted and which were human-verified
A minimum viable audit log is deliberately unglamorous: query, corpus, exclusion rule, model and prompt version, output, and human check. That is not bureaucracy. It is what makes later review possible.
If the workflow cannot generate those artifacts, the team is buying speed at the expense of defensibility.
REFRAME THE VALUE PROPOSITION
The strongest commercial and institutional message is not that our evidence pipeline is AI-enabled. The stronger message is that our evidence workflow is faster and still auditable. Senior stakeholders care about whether a process can withstand challenge, not whether it contains fashionable tooling.
RISKS, CAVEATS, OR OPEN QUESTIONS
Evidence ceiling: current peer-reviewed work supports cautious, task-specific use. It does not support a blanket claim that LLMs can automate evidence workflows without human oversight.
Evaluation gap: high publication volume does not imply prospective, decision-grade validation.
Regulatory wording risk: FDA's NAM guidance is draft and non-binding. It should not be translated into FDA acceptance language.
Operational drift: models, interfaces, and prompts can change silently over time. That is a workflow-governance problem, not just a technical detail.
WHAT ORGANIZATIONS SHOULD DO NEXT
For teams already using or planning to use LLMs in evidence work, a pragmatic 90-day agenda looks like this.
Weeks 1-2
Write a one-page Context of Use for each LLM-assisted step.
Define what the output may inform and what it may not decide.
Weeks 3-6
Version prompts and templates.
Log inputs, outputs, and human verification status.
Weeks 7-10
Measure error and variability on a representative sample.
Stress-test extraction separately from screening, because field-level reliability is not uniform.
Weeks 11-13
Package claim-to-source maps, extraction tables, exclusion logs, and a short method appendix.
Prepare a scrutiny narrative: what the workflow does, why it is fit-for-purpose, and where its boundaries sit.
EXECUTIVE TAKEAWAYS
LLMs can accelerate parts of evidence work, but the strategic bottleneck is traceability.
Screening appears more defensible as an early use case than full extraction or judgment-heavy steps.
Teams should treat each LLM-assisted step as a governed method with a clear Context of Use.
The strongest value proposition is not AI-enabled. It is audit-ready under scrutiny.
REFERENCES
FDA. General Considerations for the Use of New Approach Methodologies in Drug Development (draft guidance, March 2026; comments by 05/18/2026).
FDA. FDA Releases Draft Guidance on Alternatives to Animal Testing in Drug Development (press announcement, 18 March 2026).
Chen SF, et al. LLM-assisted systematic review of large language models in clinical medicine. Nature Medicine (published 03 March 2026).
Laignelot F, et al. Large language models show promising performance for some systematic review tasks but call for cautious implementation: a systematic review. Journal of Clinical Epidemiology (available online 12 March 2026).
Yisha Z, et al. Assessing data extraction in randomized clinical trials with large language models. BMC Medical Research Methodology (published 14 January 2026).



Comments